Languages / Idiomas / Idiomes

Home > Modification of the body-related attentional bias, through Virtual Reality, to enhance the treatment of anorexia nervosa (AN-VR-ABMT)
Modification of the body-related attentional bias, through Virtual Reality, to enhance the treatment of anorexia nervosa (AN-VR-ABMT)

Funding: This study was funded by the Spanish Ministry of Science and Innovation (Agencia Estatal
de Investigación, Ministerio de Ciencia e Innovación, Spain). Grant PID2019-108657RB-I00 funded
by MCIN/AEI/10.13039/501100011033.
This study was possible thanks to the collaboration with the Eating Disorders Unit of the Mental Health Area of the Sant Joan de Déu Hospital in Barcelona. Thanks to all the center staff for their valuable collaboration in the project.
Introduction
Anorexia nervosa (AN) is an eating behavior disorder (ED) characterized by low weight (less than 85% of what is expected considering age and height), body image disturbances and extreme fear of gaining weight (APA, 2013). In addition to the disorder's own symptomatology, AN presents a multitude of medical complications derived from the state of malnutrition, high mortality rates and high comorbidity with other disorders, especially anxiety, depressive and personality disorders. Despite the existence of different types of intervention, there is consensus that the priority in the treatment of AN is the recovery of a healthy weight and addressing the physical complications associated with underweight. Among the goals of intervention, therefore, are weight restoration, normalization of hunger and satiety perceptions of hunger and satiety, normalization of eating patterns and overcoming malnutrition through refeeding programs. However, the extreme fear of weight gain and becoming obese, characteristic of people with AN, often produces great resistance towards normalization of intake and makes it difficult for patients to reach a healthy weight. Patients with with AN often show anxiety towards certain stimuli (such as food or the body itself) and engage in avoidance behaviors (such as food restriction). Therefore, treatment of AN can be enhanced by incorporating components that target the anxiety experienced by patients while eating and face to weight gain. This is why exposure techniques have been proposed as an effective treatment in this disorder (Hildebrandt, Bacow, Greif, & Flores, 2014; Hildebrandt, Bacow, Markella, & Loeb, 2012; Steinglass et al., 2012).
Also similar to what occurs in anxiety disorders, there is a large number of studies showing the presence of attentional biases in patients with EDs and, in particular, in patients with AN. Among this diversity of research, our group has been the first (Porras-Garcia et al., 2018; Porras-Garcia et al., 2019), and to date the only one, to use virtual reality (VR) techniques in combination with eye-tracking (ET) techniques to investigate the presence of attentional biases towards the body. The synergy between these two technological resources offers opportunities that are of great interest for the study, by means of objective indicators (such as those offered by ET instruments) in highly controlled situations and with high ecological validity (such as those achievable by VR techniques), of basic processes altered in EDs, and also, relevantly, for the design of new treatment components that allow to improve the efficacy of currently available interventions for EDs; in particular, for AN.
Combined use of Eye Tracking and Virtual Reality techniques
The methods that have been used to evaluate attentional bias in patients with ED are very diverse, the most frequent being those based on modified Stroop tasks, dot-probe, visual search and eye-tracking (ET). Also, although to a lesser extent, other methods have been used, such as dichotic listening, lexical decision, and spatial pointing tasks. A complete review of these methods and the main results obtained can be found in Jiang and Vartanian (2018). Of all these techniques, ET is the only one that allows obtaining a continuous measure of the attention dedicated to different stimuli. On the other hand, with few exceptions, most cognitive tasks involve verbal stimuli, while ET techniques allow attentional behavior to be analyzed directly on visual stimuli, more directly related to the stimuli that in natural situations provoke dysfunctional responses of the patients with ED. With the ET technique, among other variables, the first fixation point, the proportion of time spent observing each stimulus, the orientation speed (through saccadic movements), or the frequency of fixations can be quantified; offering the possibility of obtaining objective measures of the location of attention. This technique therefore facilitates the objective and direct measurement of attentional biases, while cognitive tasks such as the others mentioned above only allow these biases to be inferred from response latencies. The ET technique, on the other hand, facilitates the decomposition of visual behavior into factors that are under voluntary control and factors less susceptible to that type of control, which allows us to differentiate, with greater validity than other methods, between orientation responses. automatic (vigilance), voluntary attention responses (maintenance of attention), and avoidance responses, as well as establishing their time course.
Although the ecological validity of the evaluation of attentional biases using ET is greater than with other methods, this validity can be increased even more if this technology is combined with another, such as virtual reality, which allows carrying out the evaluation of visual attention while the participant is immersed in virtual simulations of natural situations (Hans-Martin Lutz et al., 2017). With VR, in addition, one of the problems that appear in studies in which the evaluation of attentional biases towards the body is carried out using the image reflected in a mirror is solved, and that is that the patient must replace her usual clothing by tight-fitting garments or that allow observation of one's own body without distortions due to clothing. This can produce feelings of discomfort in the patient that contaminate the results, since she must show her body in these conditions to the therapists or researchers who are conducting the study. By using VR, the patient does not need to change her wardrobe during the treatment sessions, since the avatar's characteristics are defined by the program and are independent of the clothing she wears at all times.
Video: Example of eye tracking during a body exposure, processed by OGAMA.
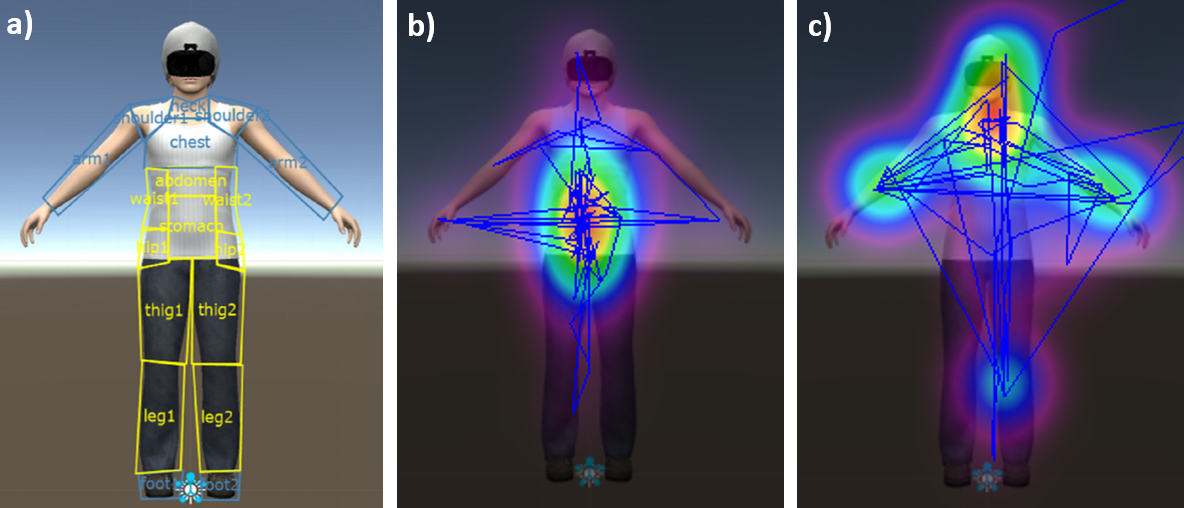
Figure: a) Definition of the areas of interest: weight-related areas in yellow, non-weight-related areas in blue. Examples of some heatmaps of attentional patterns processed by OGAMA from the eye tracking function integrated into the Virtual Reality head-mounted display: b) example of attentional bias towards weight-related areas; c) example of attentional bias towards non-weight-related areas.
Modification of attentional bias related to the body through Virtual Reality
Although research on the presence of attentional biases in EDs is extensive, very little has been done to date to apply the information obtained in these studies with the aim of improving the effectiveness of available treatments. Among the few investigations carried out in this line are those by Cardi et al. (2015) and Turton, Cardi, Treasure, and Hirsch (2017), on reducing negative biases in the interpretation of social stimuli in patients with AN; and those of Boutelle, Monreal, Strong, and Amir (2016), and Schmitz and Svaldi (2017) with patients with binge eating disorder. The modification of attentional biases toward the body, in particular, has not yet been explored in patients with AN or in patients with other EDs. Although mirror exposure is frequently used to intensify cognitive-behavioral therapy (CBT), its application is aimed at extinguishing negative cognitive, emotional, and behavioral responses to one's own body (Fairburn et al., 2008), rather than to directly modify attentional processes (Renwick et al., 2013).
Taking into account the current state of knowledge, described in the previous sections, the question arises: is it possible to improve the effectiveness of the treatment of exposure to one's own body, in patients with AN, through training aimed at modifying the attentional biases they show? If the results confirm the possibility of increasing the effect of exposure treatment to reduce anxiety and fear of gaining weight in patients with AN, as a result of the modification of attentional bias, there will be a new therapeutic resource to improve the available treatments for AN, and adapt them to a greater number of patient profiles. This objective is consistent with the growing interest in what has been called “stratified medicine”, whose purpose is to adapt treatments to the individual profiles of patients (Lester and Eley, 2013).
To reduce attentional bias, a training is applied based on an adaptation of the bias induction procedure of Smeets, Jansen and Roefs (2011). It is a procedure that has shown its effectiveness in producing changes in attentional biases in healthy participants with different levels of body dissatisfaction. This procedure was adapted to produce a reduction in bias, rather than an induction of bias toward some parts of the body or others. The result, therefore, is not greater attention to certain parts of the body (e.g. attractive or unattractive, weight-related or not), but a balanced distribution of attention between different parts of the body. Furthermore, the procedure was adapted for use with VR Head-Mounted Displays (HMD) and with ET devices integrated into them, so that the training is carried out while the patient observes, through immersive VR, an avatar that corresponds to the simulation of your own image reflected in a virtual mirror. Training is carried out by selecting geometric figures (e.g. square, rectangle, circle) that approximately fit specific parts of the body. Each of these figures can have different colors. The patient must detect and identify the figures that appear in different parts of the avatar's body. The image of the avatar is tinted using a filter that reduces its sharpness by 75%, so that the patient sees a blurred image. In half of the studies, participant must discriminate the shape of the figure and in the remaining 50% the discrimination is based on color.The change in the discrimination task (shape, color) is intended to maintain motivation to perform the task. Through the ET device, changes were programmed in the avatar so that, as soon as the participant focuses her gaze on the part of the body on which the test stimulus is located (the geometric figure), the filter that reduces the sharpness of that part of the body, making it stand out from the rest of the avatar's body. The highlight stays that way for four seconds. The patient is instructed to keep his gaze on the highlighted part until the start of the next study (four seconds). Throughout the training, the test stimulus appears on some of the body parts related to weight in 45% of the studies, and in another 45% of the studies it appears on some of the body parts not related to weight. In the remaining studies (10%), the test appears on one of the three neutral stimuli located next to the avatar, outside his body (in this case, some boxes).
Reference: Smeets, E., Jansen, A., y Roefs, A. (2011). Bias for the (un) attractive self: On the role of attention in causing body (dis)satisfaction. Health Psychology, 30(3), 360.
Video: Attentional Bias Modification Task (ABMT), adapted from Smeets, Jansen, and Roefs (2011) for the project's immersive virtual reality environment.
Hypotheses and objectives
The starting hypothesis of the project is the following:
If a component of virtual-reality-based exposure to the body image, intensified through the production of the illusion of ownership of the virtual image, is added to the usual treatment of anorexia nervosa, then the treatment will be more effective. If, in addition, a virtual-reality-based component of attentional bias reduction toward the body is added, then the treatment will further increase its efficacy.
The general objectives are:
1) To develop a procedure for the reduction of attentional biases towards the body by means of ET and VR techniques.
2) To integrate this procedure in a treatment of exposure to the body aimed at reducing the fear of gaining weight suffered by patients with Anorexia Nervosa.
3) To analyze the increase in efficacy of the usual treatment by intensifying it with the addition of a body-exposure component and by the addition of an attentional bias reduction component.
The specific objectives are:
- 1.- To develop virtual reality environments, which can be presented via HMD with ET to expose patients with AN to virtual representations of their own body shape that can be modified to simulate progressive increases in the body mass index.
- 2.- To adapt the attentional bias modification procedure of Smeets, Jansen and Roefs (2011) to be used to reduce biases towards the body in patients with anorexia, by means of ET and VR techniques.
- 3.- To test the functioning of the program developed in specific objective 2 by means of its application in people without ED with different degrees of body dissatisfaction.
- 4.- To carry out the necessary modifications in the program developed in specific objective 2, after the analysis of the results of the pilot study corresponding to objective 3.
- 5.- To test the functioning of the modified program in specific objective 4 through a pilot study conducted with patients with AN. Both its general functioning and its capacity to reduce the attentional bias towards the body will be examined.
- 6.- To make the necessary modifications to the program, after analyzing the results of the pilot study corresponding to objective 5.
- 7.- To carry out a randomized controlled clinical study to analyze the efficacy of an intensification of the usual treatment of AN by adding a component of exposure to one's own body and a component of attentional bias reduction.
- 8.- To elaborate an intervention protocol, including a clinical manual for patients with anorexia based on the results of the study carried out to achieve objective 7.
- 9.- To design and publish a web site for the free dissemination of the virtual environments and procedures developed in the project.
- 10.- To disseminate the results of the studies carried out through scientific publications with impact index and presentations at conferences.
Publications
Clinical study:
Abstract: Pending publication, available soon.
Authors: Mariarca Ascione, Eduardo Serrano-Troncoso, Marta Carulla-Roig, María Teresa Mendoza-Medialdea, Franck-Alexandre Meschberger- Annweiler, Anna Blasco Martínez, Fernando Guerrero Álvarez, Marta Ferrer-Garcia, Manuel Moreno-Sánchez, Bruno Porras-Garcia, and José Gutierrez-Maldonado
Abstract: Attentional bias modification training (ABMT) is an effective technique for reducing the dysfunctional body-related attentional bias (AB) that may be responsible for reducing the effectiveness of mirror exposure therapy (MET), which has been proposed as an effective treatment for anorexia nervosa (AN). This multiple-case study provides evidence of the usefulness of incorporating ABMT into virtual reality (VR) and eye-tracking (ET)-based MET to improve its efficacy in the treatment of four female adolescents with AN. Over five exposure sessions, patients were immersed in a virtual environment and were embodied in a real-size body virtual avatar reflected in a mirror that gradually increased body mass index (BMI) until reaching a healthy BMI in the last session. In every session, the participants completed the ABMT followed by the MET. This augmentation of MET using VR-ET-based ABMT achieved promising results for targeting AN symptomatology by reducing body dissatisfaction, drive for thinness, weight-related body parts anxiety, body checking behaviors, fear of gaining weight, and anxiety, and increasing body appreciation. Two patients who did not show a reduction in fear of gaining weight during the sessions also showed high anxiety levels, which could have affected its reduction. To advance this preliminary study and evaluate the effectiveness of incorporating ABMT into MET, a controlled clinical trial will be conducted.
Authors: Mariarca Ascione, Marta Carulla-Roig, Helena Miquel-Nabau, Franck-Alexandre Meschberger-Annweiler, Eduardo Serrano-Troncoso, Marta Ferrer-Garcia and José Gutiérrez-Maldonado
Journal: Annual Review of Cyberherapy and Telemedicine 2023 (pp. 33-39)
Year: 2023
Abstract: This case study explores the potential of integrating attentional bias modification training
(ABMT) with mirror exposure therapy (MET), utilizing virtual reality and eye-tracking, for a 14-yearold
girl diagnosed with anorexia nervosa (AN). The ABMT-MET intervention was used alongside a
standard treatment program called Home Treatment (HoT), which combines cognitive behavioral
therapy with family-based therapy. Though the patient began HoT with a 3-week inpatient phase,
the ABMT-MET intervention specifically took place during the subsequent Home Treatment sessions.
The experimental treatment, comprising five consecutive weekly sessions, was bookended by preand
post-assessment sessions and included a six-month follow-up. During the sessions, the patient
engaged in systematic and hierarchical exposure to a virtual representation of her silhouette, with
gradual adjustments made to the avatar’s body mass index (BMI) toward a healthier range. ABMT
sessions, conducted before each MET session, aimed to redistribute the patient’s focus evenly across
her body, successfully neutralizing her initial attentional bias toward non-weight-related body
parts. The patient demonstrated consistent decreases in anxiety and fear of weight gain, effectively
progressing through the BMI hierarchy in the virtual setting. Post-treatment assessments indicated
significant enhancements in body dissatisfaction, drive for thinness, body-checking behaviors, and
body appreciation, with these gains preserved at the six-month follow-up, although the attentional
bias returned to pre-treatment levels. Though the single-case design limits definitive conclusions,
these findings suggest ABMT-MET may be a promising adjunct therapy for AN, requiring further
research for confirmation.
Authors: Mariarca Ascione, Eduardo Serrano-Troncoso, Marta Carulla-Roig, Anna Blasco Martínez, Fernando Guerrero Álvarez, Franck-Alexandre Meschberger-Annweiler, Bruno Porras-Garcia, Marta Ferrer-Garcia and José Gutierrez-Maldonado
Journal: Applied Sciences
Year: 2024
Abstract: Pending publication, available soon.
Authors: Franck-Alexandre Meschberger-Annweiler, Marta Carulla-Roig, Mariarca Ascione, Bruno Porras-Garcia, Eduardo Serrano-Troncoso, Marta Ferrer-Garcia and José Gutierrez-Maldonado
Pilot studies, optimization of the experimental protocol and the Virtual Reality system:
Abstract: Mirror exposure therapies (METs) have been shown to be effective in reducing body image
disturbances through the habituation process. Virtual reality (VR) combined with eye-tracking
techniques can provide innovative solutions to some of METs’ limitations reported with patients
with anorexia nervosa (AN), especially the negative influence of body-related attentional bias (AB).
This pilot study aimed to assess the preliminary efficacy of a new VR-based AB modification task
(ABMT) among healthy women and the procedure’s user experience. AB levels towards weight- and
non-weight-related body parts, using complete fixation time (CFT) and number of fixations (NF),
were assessed throughout the ABMT procedure (300 trials). The user experience was evaluated at
the end of the procedure. The results showed that VR-based ABMT was effective in reducing AB
significantly after 150 trials for both CFT- and NF-based measures, although 225 trials were necessary
to get the same result for women with an NF initially more oriented towards weight-related body
parts. Overall, the software received a “C-rating” on a scale from “A” (most usable) to “F” (least
usable). These results provide evidence of the opportunity to use a VR-based ABMT procedure to
reduce AB and improve existing treatments for AN.
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Bruno Porras-Garcia, Marta Ferrer-Garcia,
Manuel Moreno-Sanchez, Helena Miquel-Nabau, Eduardo Serrano-Troncoso, Marta Carulla-Roig and José Gutiérrez-Maldonado
Journal: Journal of Clinical Medicine
Year: 2023
Abstract: Anorexia nervosa (AN) patients exhibit attentional bias (AB) related to the body, which is the tendency to pay greater attention to weight-related body areas compared to non-weight-related ones. This phenomenon has been linked to elevated levels of body dissatisfaction (BD) and may potentially reduce the effectiveness of body exposure therapy. The purpose of this pilot study is to assess the efficacy of a single session of a new body- related AB modification task (ABMT) that combines virtual reality with eye tracking in patients with AN. The goals of the ABMT are to reduce body-related AB by balancing attention between weight and non-weight-related body areas and to reduce BD levels. Twenty-three adolescent patients with AN were embodied in a virtual avatar and immersed in a virtual environment where they completed the ABMT. Body-related AB measures and BD levels were assessed before and after the training. A paired samples t-test showed statistically significant differences between pre-assessment and post-assessment; the complete fixation time on weight-related body parts was reduced and BD levels decreased. The initial evidence of the efficacy of this ABMT has important clinical implications, since AB and BD are considered risk factors for developing and maintaining eating disorder symptomatology among patients with AN.
Authors: by Mariarca Ascione, Marta Carulla-Roig, Helena Miquel-Nabau, Bruno Porras-Garcia, Franck-Alexandre Meschberger-Annweiler, Eduardo Serrano-Troncoso, Marta Ferrer-Garcia, Manuel Moreno-Sánchez and Jose Gutierrez-Maldonado
Journal: Journal of Clinical Medicine
Year: 2023
Abstract: Recent technological advances have paved the way for incorporating virtual reality (VR)
into attentional bias modification training (ABMT) for the treatment of eating disorders. An important
consideration in this therapeutic approach is ensuring the ease and comfort of users of the hardware
and software, preventing them from becoming additional obstacles during treatment. To assess
this, 68 healthy participants engaged in an ABMT experiment aimed at evaluating various factors,
including usability as well as the participants’ comfort while using the VR equipment, task-induced
fatigue, and attitudes towards the technology. Our results indicated a favorable usability level for
the ABMT proposed in this study. While their discomfort, anxiety, and fatigue increased during the
task, these did not significantly impact its execution. However, heightened anxiety and fatigue were
linked to lower evaluations of software usability. Other variables considered in the experiment did
not notably affect the task.
Authors: María Teresa Mendoza-Medialdea, Ana Carballo-Laza, Mariarca Ascione,
Franck-Alexandre Meschberger-Annweiler, Bruno Porras-Garcia, Marta Ferrer-Garcia and José Gutiérrez-Maldonado
Journal: Applied Sciences
Year: 2023
Abstract: Cognitive biases have a significant impact on the etiology and treatment of eating disorders
(EDs). These biases, including selective attentional bias (AB) to disliked body parts, may reinforce
concerns about body shape, fear of gaining weight and body image disturbances and may contribute
to dietary restriction and restraint. Decreasing AB could reduce core symptoms in anorexia nervosa
(AN). This study represents a preliminary exploration aiming to assess whether AB towards weightrelated
(WR) and non-weight-related (NW) body parts could be reduced through an AB modification
task in a virtual reality (VR) environment in healthy participants. A total of 54 female participants
were recruited. The task consisted of directing the participants’ attention towards
all body parts equally in a VR setting. Eye-tracking (ET) measurements (complete fixation time [CFT]
and number of fixations [NF]) were made before and after the task. The results showed a significant
reduction of the AB in the two groups with an initial AB towards WR body parts or towardsNWbody
parts. Participants showed a tendency to more balanced (non-biased) attention after the intervention.
This study provides evidence of the usefulness of AB modification tasks in a non-clinical sample.
Authors: Helena Miquel-Nabau, Natalia Briseño-Oloriz, Bruno Porras-Garcia, Mariarca Ascione, Franck-Alexandre Meschberger-Annweiler, Marta Ferrer-Garcia, Manuel Moreno-Sanchez, Eduardo Serrano-Troncoso, Marta Carulla-Roig and José Gutiérrez Maldonado
Journal: Brain Sciences
Year: 2023
Deepening the theoretical knowledge related to the project:
Abstract: Previous research has shown an association between body dissatisfaction and attentional
biases toward the body, but the nature of this relationship is not clear. It is possible that dissatisfaction
causes attentional bias or that dissatisfaction is a result of such bias. To clarify the causal relationship
between these two variables, this study manipulated dissatisfaction in a sample of healthy
women by exposing them to images of “ideal” bodies and observed whether this manipulation
increased attentional biases toward different body parts. Fifty-seven women took part in a pre–post
experimental design in which they observed an avatar representing themselves in a virtual mirror
before and after being exposed to “thin ideal” photographs. Eye-tracking technology was employed
to quantify the frequency and duration of fixations on weight-related and weight-unrelated body
parts. The outcomes revealed a successful induction of body dissatisfaction, leading participants to
display a heightened number of fixations and prolonged fixation durations on unrelated-weight body
parts. These findings remained significant after controlling for the effects of trait body dissatisfaction
and body mass index. The results imply that heightened body dissatisfaction fosters the aversion
of attention from weight-related body parts, which may function as a protective mechanism for
preserving self-esteem and promoting psychological well-being.
Authors: María Teresa Mendoza-Medialdea, Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Alejandra Rueda-Pina, Elisa Rabarbari, Bruno Porras-Garcia, Marta Ferrer-Garcia and José Gutiérrez-Maldonado
Journal: Journal of Clinical Medicine
Year: 2023
Abstract: Anorexia nervosa (AN) is a severe disorder. It has higher mortality rates than other eating disorders (ED) and is increasingly being diagnosed in younger patients. One of the main fears among individuals with AN is the fear of gaining weight (FGW). Patients with AN also display dysfunctional behaviors that aim to avoid weight gain by drastically reducing food intake, vomiting, using laxatives and diuretics, or doing intense exercises. AN patients engage in frequent conduct of checking and scrutinizing those parts of their body directly related with weight, which suggests attention focused on the body that has a dysfunctional nature. Although research on the presence of attentional biases in ED is extensive, very little has been done up to the present to apply the information gathered in those studies with the purpose of improving the efficacy of the available treatments. One of our recent projects aimed to provide evidence of the efficacy of a virtual reality-based body exposure therapy in AN in directly targeting the FGW through a randomized controlled clinical trial. We are currently developing a new clinical trial to test whether the addition of a component aimed at reducing the attentional bias towards the body serves to intensify the effect of the exposure treatment. It is expected that the reduction of the attentional bias will facilitate the control of visual avoidance behaviors during exposure sessions, increasing the efficacy of the treatment.
Authors: Jose Gutierrez-Maldonado, Natalia Briseño, Mariarca Ascione, Franck Meschberger-Annweiler, Bruno Porras-Garcia, Marta Ferrer- Garcia, Eduardo Serrano and Marta Carulla
Journal: HCII 2023: Virtual, Augmented and Mixed Reality pp. 453–463
Year: 2023
Abstract: Body dissatisfaction, fear of gaining weight (FGW) and body anxiety have been extensively studied as some of the strongest risk and maintenance factors of anorexia nervosa (AN) symptomatology. Recently, a new theoretical model introduced self-disgust as a factor that can lead to avoidance behaviors when patients with AN face their body. This can make them vulnerable to relapse. In addition, body-related attentional bias (AB) (e.g., selective attention to weight-related body areas) can limit the efficacy of body exposure therapies. This study aims to investigate the possible predictors of AB, to better understand the underlying mechanisms that contribute to the maintenance of AN symptomatology. A total of 116 college students from the University of Barcelona participated in the study, using a combination of virtual reality and eye-tracking techniques to provide an objective and reliable assessment of AB in a highly realistic environment. Stepwise multiple linear regression analyses were performed to identify possible predictors of AB among body mass index, FGW, body anxiety, body dissatisfaction and self-disgust. The results shows that both body dissatisfaction and self-disgust are significant predictors of AB. While an increase in body dissatisfaction predicted a greater AB towards weight-related body areas (positive regression coefficients: BBody_dissatisfaction→AB > 0, p < .001), the opposite occurred with self-disgust (negative regression coefficients: BSelf_disgust→AB < 0, p < .02). Such results provide initial evidence that self-disgust, which is a more intense negative feeling than body dissatisfaction, leads to gaze avoidance towards weight-related body areas, which are considered disgust elicitors.
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Julia Prieto-Perpiña, Chiara Verdasco, Marta Ferrer-Garcia and José Gutiérrez-Maldonado
Journal: Annual Review of Cyberherapy and Telemedicine 2023 (pp. 76-82)
Year: 2023
Abstract: Objective: This study examines the relationships between self-disgust, body dissatisfaction (BD), and attentional biases (AB) toward weight-related body areas, exploring whether self-disgust predicts attentional avoidance and moderates the relationship between BD and AB.
Method: Using virtual reality and eye-tracking technology, 78 female students viewed their virtual bodies in a mirror to assess gaze patterns as an indicator of attentional bias. Results: BD was positively associated with both AB and self-disgust. Contrary to expectations, self-disgust correlated with increased
attention to weight-related areas rather than avoidance and did not moderate the BD–AB relationship. Discussion: These findings suggest that self-disgust may reinforce attention toward weight-related areas, contributing to negative body image. Future research should explore these mechanisms in clinical populations to inform targeted interventions.
Authors: Mariarca Ascione, Klaske A. Glashouwer, Franck-Alexandre Meschberger-Annweiler, Teresa Mendoza-Medialdea, Bruno Porras-Garcia, Marta Ferrer-Garcia and José Gutierrez-Maldonado
Journal: International Journal of Eating Disorders
Year: 2025
Abstract: Background: Body dissatisfaction (BD) has been consistently linked to adverse consequences
on mental health and overall well-being, and is recognized as a significant contributing factor
in the initiation and persistence of eating disorders (EDs). Empirical evidence has demonstrated that
an elevated body mass index (BMI) and media influence and pressure about a thin ideal heighten
the risk of subsequent BD. Moreover, suggestibility, a propensity to accept and act upon messages
without critical evaluation, has been shown to be positively associated with greater susceptibility
to the influence of sociocultural messages that endorse the thin ideal. This study aimed to assess
whether suggestibility moderates the association between BMI and BD in women. Methods: A total
of 117 women completed assessments using the Eating Disorder Inventory-3 (EDI-3) BD subscale and
the Suggestibility Inventory, which encompasses a general suggestibility index and a subscale that
evaluates susceptibility to influence by others. We conducted moderation analyses employing the
PROCESS macro, with BMI as the central predictor, BD as the outcome variable, and suggestibility
and its subscale as moderators. Results: The findings revealed statistically significant positive moderating
interactions for both the general suggestibility index and susceptibility to influence by others.
Specifically, women who exhibited high levels of suggestibility and susceptibility to influence by
others demonstrated a more pronounced increase in BD as their BMI increased. Conclusions: These
outcomes are in line with the sociocultural model of EDs, suggesting that greater susceptibility to
external influences amplifies the impact of societal pressures to conform to thin ideals.
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Bruno Porras-Garcia, Maria-Teresa Mendoza-Medialdea, Marta Ferrer-Garcia and Jose Gutierrez-Maldonado
Journal: Journal of Clinical Medicine
Year: 2024
Abstract: Pending publication, available soon.
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Bruno Porras-Garcia, Maria-Teresa Mendoza-Medialdea, Eduardo Serrano- Troncoso, Marta Carulla-Roig, Marta Ferrer-Garcia, and Jose Gutierrez-Maldonado
Abstract: The application of advanced embodied technologies, particularly virtual reality (VR), has been suggested as a means to
induce the full-body illusion (FBI). This technology is employed to modify different facets of bodily self-consciousness,
which involves the sense of inhabiting a physical form, and is influenced by cognitive inputs, affective factors like body dissatisfaction,
individual personality traits and suggestibility. Specifically, VR-based Mirror Exposure Therapies are used for
the treatment of anorexia nervosa (AN). This study aims to investigate whether the “Big Five” personality dimensions, suggestibility,
body dissatisfaction and/or body mass index can act as predictors for FBI, either directly or acting as a mediator,
in young women of similar gender and age as most patients with AN. The FBI of 156 healthy young women immersed in VR
environment was induced through visuomotor and visuo-tactile stimulations, and then assessed using the Avatar Embodiment
Questionnaire, comprising four dimensions: Appearance, Ownership, Response, and Multi-Sensory. Data analysis encompassed
multiple linear regressions and SPSS PROCESS macro’s mediation model. The findings revealed that the “Big Five”
personality dimensions did not directly predict FBI in healthy young women, but Openness to experience, Agreeableness,
and Neuroticism exerted an indirect influence on some FBI components through the mediation of suggestibility.
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Bruno Porras-Garcia, Maria-Teresa Mendoza-Medialdea, Julia Prieto- Perpiña, Adela Fuste-Escolano, Jose Ruiz-Rodriguez, Marta Ferrer-Garcia, and Jose Gutierrez-Maldonado
Journal: Virtual Reality (Springer)
Year: 2024
Abstract: Pending publication, available soon.
Authors: Helena Miquel-Nabau, Bruno Porras-Garcia, Mariarca Ascione, Franck-Alexandre Meschberger-Annweiler, Marta Ferrer-Garcia, Manuel Moreno-Sanchez, Eduardo Serrano-Troncoso, Marta Carulla-Roig and Jose Gutierrez Maldonado
Abstract: According to recent research, eating disorder (ED) patients tend to check unattractive body parts. However, few studies have studied this attentional bias (AB) phenomenon combining virtual reality (VR) with eye-tracking (ET). This study aims to examine whether anorexia nervosa (AN) patients have a longer fixation time and a greater fixations number on the weight-related body areas compared to the healthy sample with high body dissatisfaction (HBD) and low body dissatisfaction (LBD). It will also examine whether the HBD group will have more fixations and spend more time looking at weight-related areas than those with LBD. Forty-three college women (18 with HBD and 25 with LBD) and 23 AN patients were immersed in a virtual environment and then embodied in a virtual avatar with their real body measurements and body mass index (BMI). Eye movement data were tracked using an ET device incorporated in the VR headset (FOVE). The number of fixations and the complete fixations time were registered on the weight-related areas of interest (W-AOIs) and non- weight-related areas of interest (NW-AOIs). The results showed that AN patients have a longer fixation time and a greater fixations number on W-AOIs than both HBD and LBD groups, who did not show any statistical differences in the visual selective attention to NW-AOIs and W-AOIs.
Authors: José Gutierrez-Maldonado, Mar Clua i Sánchez, Bruno Porras-Garcia, Marta Ferrer-Garcia, Eduardo Serrano, Marta Carulla, Franck Meschberger-Annweiler and Mariarca Ascione
Journal: HCII 2022: Virtual, Augmented and Mixed Reality pp. 443-454
Year: 2022
Authors: José Gutiérrez-Maldonado
Journal: Journal of Clinical Medicine (Editorial)
Year: 2022
Abstract: Pending publication, available soon.
Autores: María Teresa Mendoza-Medialdea, Pau Vallès-Jaén, Mariarca Ascione, Franck-Alexandre Meschberger-Annweiler, Bruno Porras-Garcia, Marta Ferrer-García and José Gutiérrez-Maldonado
Abstract: Pending publication, available soon.
Authors: María Teresa Mendoza-Medialdea, Anil Nanwani-Vazquez, Mariarca Ascione, Franck-Alexandre Meschberger-Annweiler, Bruno Porras- Garcia, Marta Ferrer-García1 and José Gutiérrez-Maldonado
Posters and oral presentations at conferences
Download the posters and oral presentations at conferences, carried out within the framework of this project:
Authors: Mariarca Ascione, Marta Carulla-Roig, Franck-Alexandre Meschberger-Annweiler, Eduardo Serrano-Troncoso, Marta Ferrer-Garcia and Jose Gutierrez-Maldonado
Conference: XXXth Annual Meeting of the Eating Disorders Research Society
City and dates: Sitges, September 26-28, 2024
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Marta Carulla-Roig, Helena Miquel-Nabau, Eduardo Serrano-Troncoso, Marta Ferrer-Garcia and Jose Gutierrez-Maldonado
Conference: VR Mental Health Conference 2023
City and dates: Groningen, November 9-10, 2023
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Maria-Teresa Mendoza-Medialdea, Marta Ferrer-Garcia and Jose Gutierrez-Maldonado
Conference: VR Mental Health Conference 2023
City and dates: Groningen, November 9-10, 2023
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Julia Prieto-Perpiña, Chiara Verdesca, Marta Ferrer-Garcia and José Gutierrez-Maldonado
Conference: 26th Annual Cyberpsychology, Cybertherapy and Social Networking Conference (cypsy26)
City and dates: Paris, July 11-13, 2023
Authors: Ascione M., Carulla-Roig M., Miquel-Nabau H., Meschberger-Annweiler F.A., Serrano-Troncoso E.,Ferrer-Garcia M.,Gutierrez. Maldonado J.
Conference: 26th Annual Cyberpsychology, Cybertherapy and Social Networking Conference (cypsy26)
City and dates: Paris, July 11-13, 2023
Authors: Ascione M., Carulla-Roig M., Miquel-Nabau H., Meschberger-Annweiler F.A., Serrano-Troncoso E., Porras-Garcia B.,Ferrer-Garcia M., Gutierrez-Maldonado J.
Conference: International Congress of Eating Disorders (ICED) 2023
City and dates: Washington, June 1-3, 2023
Authors: Ascione M., Carulla-Roig M., Miquel-Nabau H., Meschberger-Annweiler F.A., Serrano-Troncoso E., Porras-Garcia B.,Ferrer-Garcia M., Gutierrez-Maldonado J.
Conference: International Congress of Eating Disorders (ICED) 2023
City and dates: Washington, June 1-3, 2023
Authors: Franck-Alexandre Meschberger-Annweiler, Mariarca Ascione, Bruno Porras-Garcial, Helena Miquel, Erik Exposito, Eduardo Serrano-Troncoso, Marta Carulla-Roig, Marta Ferrer-Garcia, Jose Gutierrez-Maldonado
Conference: European Congress of Psychiatry - EPA 2023
City and dates: Paris, March 25-28, 2023
Authors: Ascione M., Carulla-Roig M., Miquel-Nabau H., Meschberger-Annweiler F.A., Serrano-Troncoso E.,Ferrer-Garcia M.,Gutierrez. Maldonado J.
Conference: 2nd Brain & Mind Conference
City and dates: Barcelona, March 17, 2023
Authors: Meschberger-Annweiler, Franck-Alexandre; Ascione, Mariarca; Miquel, Helena; Porras-Garcia, Bruno;
Exposito, Erik; Serrano-Troncosa, Eduardo; Carulla-Roig, Marta; Ferrer-Garcia, Marta; Gutierrez-Maldonado, Jose
Conference: International Multi-Brain Congress
City and dates: Barcelona, November 9-10, 2022
Authors: Ascione M., Carulla-Roig M., Miquel-Nabau H., Meschberger-Annweiler F.A., Serrano-Troncoso E., Porras-Garcia B.,Ferrer-Garcia M.,Gutierrez-Maldonado J.
Conference: International Multi-Brain Congress
City and dates: Barcelona, November 9-10, 2022
Authors: Ruiz, J., Fusté, A., Meschberger, F.A., Ascione, M., Expósito, E., Ferrer-Garcia, M. & Gutiérrez-Maldonado, J.
Conference: European Association for Behavioural and Cognitive Therapies (EABCT) Congress 2022
City and dates: Barcelona, September 7-10, 2022
Authors: Franck-Alexandre Meschberger-Annweiler, Bruno Porras-Garcia, Mariarca Ascione, Helena Miquel, Eduardo Serrano-Troncoso, Marta Carulla-Roig, Marta Ferrer-Garcia and Jose Gutierrez-Maldonado
Conference: International Congress of Eating Disorders (ICED) 2022
City and dates: Virtual event, June 9-10, 2022
Authors: Ascione M., Porras-Garcia B., Meschberger-Annweiler F.A., Miquel-Nabau H., Serrano-Troncoso E., Carulla-Roig M., Ferrer-Garcia M., Gutierrez-Maldonado J.
Conference: International Congress of Eating Disorders (ICED) 2022
City and dates: Virtual event, June 9-10, 2022
Press
Visibility of the project in the press:
Newspapers:
Newspaper: La Vanguardia
Date: May 12, 2023
----------
Television:
Network: Antena 3
Date: May 16, 2023
General conclusions
This study's results confirm the potential of Virtual Reality-based exposure therapy for improving Eating Disorders' symptoms in adolescents with Anorexia Nervosa and encourage further exploration to fully understand the impact of Attentional Bias Modification Training in Virtual-Reality-based exposure therapy.
The innovative approach, including the integration of an Attentional Bias Modification Training and personalized virtual avatars, along with its pioneering use of eye-tracking technology, holds significant promise for advancing future research and clinical practice in Eating Disorders' treatment.